Rounded Shoulders, Forward Head, And Kyphosis, Oh My! - How To Fix Upper Cross Syndrome
I’ve got a good one for you today, folks. Rounded shoulders, forward head, and kyphosis A.K.A. “upper cross syndrome” can be unsightly and make you a bit self-conscious. I remember walking into a bar back in college and my friend saying, “Dude, stand up straight.” That simple comment pierced my soul, ego, or whatever emotional thing that makes you feel like crap. The next thing I know, I’m over retracting my shoulder blades and trying anything I could do to “stand up straight.”
Okay, I digress. I’m triggered, but enough about my postural sob story. What this post will cover:
We’ll define rounded shoulders, forward head, and kyphosis (upper cross syndrome)
We’ll find out why it matters
Why’s it happen
How to fix it
Some exercises to try
Let’s dive in!
What Are Rounded Shoulders, Forward Head, And Kyphosis (Upper Cross Syndrome)?
Alright, so quick tip: all three of these positions or postures of the upper body can occur together or separately (Singla, D et al. 2017). So, let’s define each one (photo examples linked) and throw them all back together:
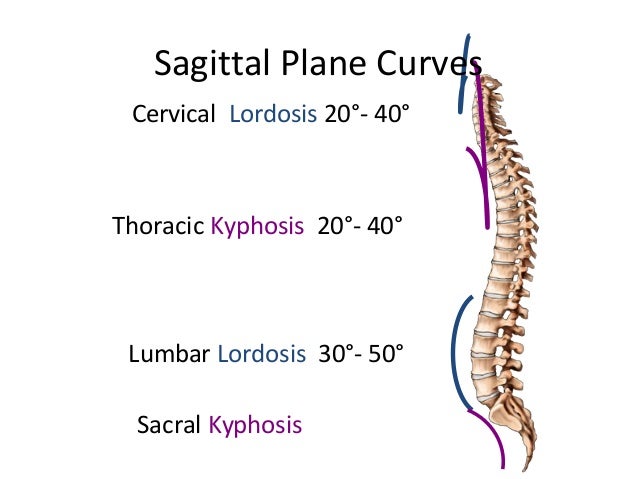
Kyphosis - The normal convex curvature of the spine that occurs at the thoracic vertebrate and sacrum (about 20°-40° at the thoracic spine).
Hyperkyphosis - “Thoracic hyperkyphosis, often referred to as kyphosis or hunchback, is described as an excessive antero-posterior curvature of the thoracic spine of greater than 40°. Normal kyphosis angles can vary between 20° and 40° in the younger public, however, in older populations, the mean kyphosis angle is 48° to 50° in women and about 44° in men.” - Physiopedia
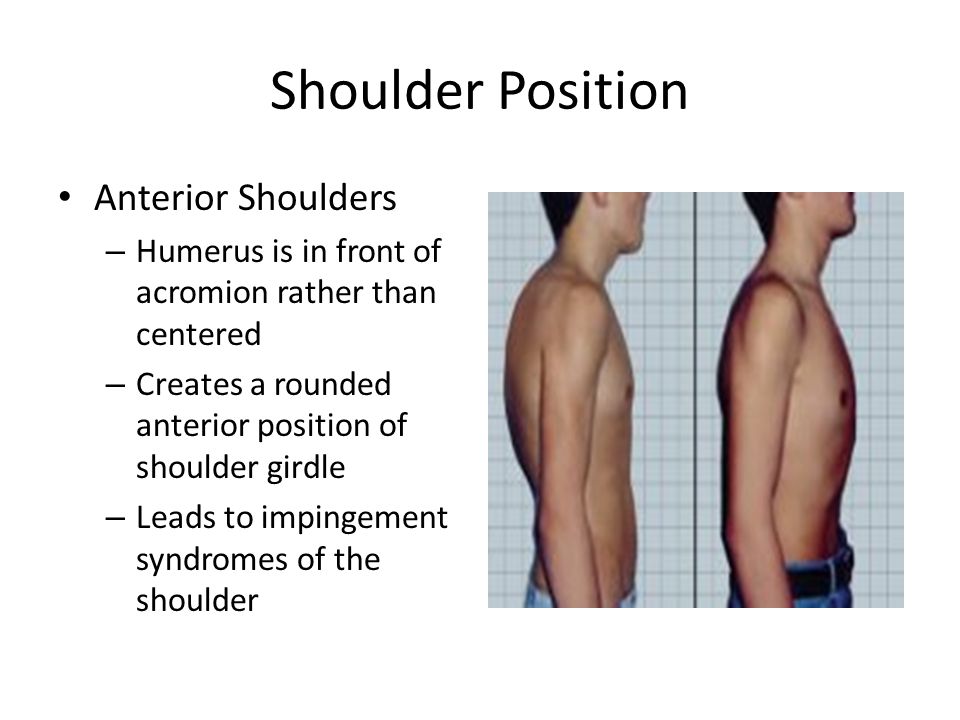
Rounded Shoulder Posture - “A posture characterized by acromion protraction in front of the line of gravity, shoulder protraction, and downward rotation as well as anterior tilt.” - Yang, H. 2013
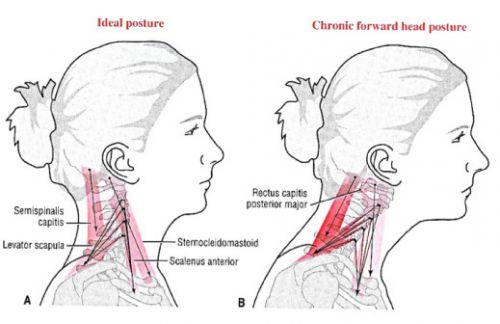
Forward Head Posture - “Increased flexion of lower cervical vertebrae and the upper thoracic regions, increased extensions of upper cervical vertebrae and extension of the occiput on C1” - Physiopedia
Upper Cross Syndrome - “Tightness of the upper trapezius and levator scapula on the dorsal side crosses with tightness of the pectoralis major and minor. Weakness of the deep cervical flexors ventrally crosses with weakness of the middle and lower trapezius” - Physiopedia
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Alright, so that’s a lot of crazy medical jargon. Let’s dissect these definitions a bit more. We’ll start with kyphosis vs. hyperkyphosis.
Kyphosis is a normal, I repeat, normal curvature of the human spine. The major region that this curvature occurs is at the thoracic spine. If we didn’t have this curvature, well we wouldn’t be able to stand upright. Oh, and our breathing wouldn’t be nearly as efficient as we wouldn’t have room for our lungs to expand properly.
Hyperkyphosis is when our normal kyphotic curvature (20°-40°) has gotten a bit out of control. You see this with an increase in the convex curvature (greater than 40°) at the thoracic spine. This is where weird things start happening to our posture (this is important so take note). So basically it’s all just a bunch of semantics. You’ll hear many people relate their hyperkyphosis to kyphosis all the time, but really the angle at which this curvature is measured is how you could truly “diagnosis” it (but just doing a posture assessment can do the trick). Okay, so now we hopefully have kyphosis and hyperkyphosis down. Let’s look at rounded shoulders and forward head postures.
Well, to be honest, they’re pretty self-explanatory. Forward head is when your chin pokes out forward leading your neck into a funky curvature out in front of the body. Rounded shoulder posture occurs when the acromion (here’s a video on how to find the acromion) is in front of the midline of the body. So that bony process points forward and down and you’ll see what sort of looks like a sunken chest.
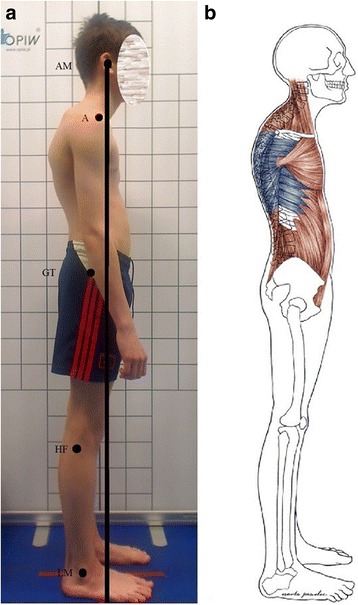
Lastly, upper cross syndrome is really a combination of all these postures. Think of it as an umbrella term as the majority of the time rounded shoulders, forward head, and hyperkyphosis occur together. Going forward in this post, we’ll use upper cross syndrome to encompass kyphosis, rounded shoulders, and forward head. The photo below really shows all of this in action along with the musculature behind the postures.
Acromion should be a little more forward, but I think you get it.
Why Does Upper Cross Syndrome Matter?
Well, for one, no one really likes this posture. It’s unappealing from a cultural perspective (I’m triggered and have flashbacks to that college bar). It’s can be associated with being unhealthy, lacking fitness, or getting older (think an 80s movie nerdy dude or gramps with his walker). But other than it being unaesthetic, this posture isn’t “bad” per se but a compensation that occurs out of necessity. If you haven’t read my post “Good Posture - What Is It?” I suggest checking it out to learn more about how we define “good” posture.
Alright, so I’m sure you went and read that post. So now you understand that upper cross syndrome may be a sign of lost movement options throughout the entire body. That it’s just a potential “compensation” posture to help keep you moving.
But, with this postural compensation, you can potentially get weird stuff like scapulohumeral rhythm issues and winged scapula where essentially the muscles are out of wack and you can’t stabilize the shoulder “optimally” due to your improper posture positioning.
Another crazy thing we see with the upper cross syndrome is hyperactivity of your oculomotor (vision and eye movement) and vestibular (balance) systems (Morningstar, M. 2005). That means your balance can be impaired (again think of grandpa and his walker), you may be more susceptible to eye strains and decreases in your vision, and overall, you’re unable to sense the world around you effectively (which is SUPER important).
How To Know If You Have Upper Cross Syndrome
So, you have a couple of options to find out if you have this posture.
Get someone to measure your kyphosis / forward head with a digital inclinometer
If you remember from the definitions, we defined normal kyphosis as being a convex curvature of 20°-40°. Anything greater than 40° is deemed hyperkyphosis.
Pros:
You have some objective measures that you can remeasure as you go through your posture journey.
It’s a pretty fast and reliable measurement
Cons:
You need someone else to take the measurement (preferably someone skilled)
The measurement can’t really yield data for rounded shoulders (as far as I know)
These tools can be pretty expensive
Do A Posture Assessment
These assessments can be easy and cheap or can get pretty expensive over time. I suggest always going cheap and easy just because, well if you’re reading this, you probably want that option. You can either use posture software which is pretty reliable and objective, but begins to be pricy or just take some photos and compare them week by week. I’ll also do some free posture assessments via Zoom for you that you can schedule here: “Free Consultation”
Posture Software Assessment
Pros:
Reliable and objective so you can retest
Can yield data on forward head, kyphosis/hyperkyphosis, and rounded shoulders
Cons:
Cost money
Potentially requires someone else to take or read the measurement
Posture Assessment By Clinician Or Self
Pros:
Easy and potentially less expensive
Can do it on yourself with a cellphone or camera
Can yield data on forward head, kyphosis/hyperkyphosis, and rounded shoulders
Cons:
Not as reliable or objective as the previous two options
In my experience, posture assessments on your own or by some sort of “expert” are best just because they’re easier. Having a skilled professional take a look can help a lot and they often will do it for free (like myself *hint* *hint*). Alright so we scratched the surface of why we should care about upper cross syndrome, but let’s keep it rolling as to why this posture occurs.
What Causes Upper Cross Syndrome?
Well, unfortunately, there’s no black or white answer as to why. If there was then I probably wouldn’t be writing this post and we’d all have perfect, amazing posture. Below we’ll dip into a couple of reasons it can occur.
Anterior Pelvic Tilt and Gravity
Visual System and Glasses
Vestibular System and Kinesthetics
Breathing and Respiratory Optimization
For the purpose of this post, we’ll cover the biomechanics of the anterior pelvic tilt and gravity as well as the visual system, as those are two primary systems I go after in terms of postural correction. The other ones are important and we still take them into consideration in the exercise portion of this post, but if I start going into detail… well we’ll be here all day. I’ll write about that stuff soon.
To preface before we dive in, these things are just scratching the surface of “why” you may have upper cross syndrome. But in reality, it’s probably some crazy complex combination of all of these with some really fun behaviors and biopsychosocial stuff sprinkled on top.
My goal is to bring attention to the true complexity of posture training and provide up to date information on these topics. Scapular squeezes and chin tucks can only get you so far.
Okay, hope that made sense.
Anterior Pelvic Tilt and Gravity
Real quick, If you’re not familiar with anterior pelvic tilt and its effect on the body, then I highly suggest you check out my last post “Anterior Pelvic Tilt - How To Fix Your Asymmetries” to bring you up to speed.
Alright, so think about the last time you played Jenga. When the bottom of the tower starts to lose support, the entire structure begins to lean in one direction due to gravity. Now our bodies are way more complicated than a stack of wooden blocks (we’ll dive into this soon). But in general, when our base of support or center of gravity is off (your pelvis), a common symptom you’ll see is a compensation up the spine (see where this is going?).
{kind=link}
So, the bottom of the Jenga tower is your pelvis stuck in an anterior pelvic tilt. The tower begins to lean to one side. Now, the tower is a simple structure and when it leans to move side far enough, gravity overwhelms the structure and it just falls. Luckily, our bodies are awesome and can compensate to fight gravity. Enter the upper cross syndrome.
So, if we look at my own posture photo, my pelvis is dumped forward and I lack the control over this bony structure to move/balance my center of gravity effectively. This may cause my low back, or lordotic curvature, to increase (think about the Jenga tower leaning). My ribcage may become compressed and my thoracic curvature may begin to exaggerate (hyperkyphosis) in order to counteract gravity and the “leaning” of my body. Basically, the top-middle of my spine curves to go the opposite direction away from the body falling forward.
{kind=link}
Well now that the top of my spine is going back, I don’t want to become top-heavy and fall backward! So, another compensation occurs, the rounding of my shoulders and forward head posture. These kick in to counteract the overcorrection of hyperkyphosis at the upper-middle region of the spine.
okay so that got a bit deep. If you get anything from this section it’s that these “compensations” and postures are defaults in “normal” healthy individuals. Think, your anterior pelvic tilt, kyphotic curvature of the thoracic spine, and forward head all are preset things in the human skeletal structure. They’re what make us adaptable and successful as a species. Really, these postures just become exaggerations of our normal positionings. The system increases its spinal curvatures in order to create a larger base of support to help us fight gravity.
Visual System and Glasses
Another big reason I see upper cross syndrome occurring is due to our eyes. Many of us are familiar with sitting for long periods of time in a “slouched” position or text neck. We think that because we’re in these positions we become stuck due to muscle becoming “tight". While that can be true I’ve found it’s not the full story. In reality, our visual system and ability to focus becomes, for a lack of better words, “stuck” decreasing our ability to sense the world around us.
Our eyes being fixed on screens for hours on hours strains the musculature in our eyes to the point where they spasm or become myopic. When you look up may then have an inability to refocus your eye on objects farther away, thus you maintain a forward head posture to bring your eyes closer to the object you’re trying to see.
“It is well known that vision has a major role in the regulation of upright posture, particularly by maintaining head position in space. Alterations in head posture may develop secondarily to visual changes. For example, Havertape and Cruz showed how the addition of eyeglasses changed the head position in 5 patients with a chin-down posture as a result of high hyperopia. Likewise, Willford et al showed that people who wear prescription multifocal lenses tend to exaggerate a forward head posture to utilize the proper area of the lens, depending upon the functional needs of the moment.” (Morningstar, M. 2005)
Pretty crazy, right? In my experience in both fixing my own posture and helping clients, folks with poor vision tend to have visually “worse” posture (upper cross syndrome), especially those that have suffered concussions.
How To Fix Upper Cross Syndrome?
Alright, here’s the part where we provide some solutions to what I have definitely overcomplicated above. We’ll break these exercises up into musculature biomechanics (think anterior pelvic tilt, tight pecs, etc.) and ones that go after the visual system.
Breathing Exercises
90-90 Hip Lift
EQUIPMENT:
Your floor
A chair or wall
(Optional) Pillow
(Optional) yoga block, ball, or towel between the knees
SET-UP:
Lay down on your back with your legs at 90 degrees and feet against the wall
(Optional) Place a pillow under your head and neck
Place the hands on the lower portion of your ribs (where you feel them stick out a little)
Feel the heels of your feet pull down on the wall like your scraping paint (feel hamstrings)
Gently tuck your back pockets toward the back of your knees (posterior pelvic tilt) leaving belt line on the floor
Hold the yoga block between the knees with a gentle squeeze
Maintain set up throughout execution
EXECUTION:
Exhale every spit of air you got in the tank out through the mouth
Feel your lower abdominals around your belt line turn on while the lower ribs fall down and back toward the spine
Hold breath at the end of the exhale with your tongue against the roof of your mouth for 3-5 seconds
Maintain abdominal tension and lower ribs down while silently inhaling through the nose with the tongue still against the roof of the mouth
Feel expansion throughout front and sides of the ribcage
Repeat for recommended sets and reps
ADDITIONAL TIPS:
When the abs or lower ribs start to move, that’s your cue to start exhaling again
Keep your neck and face relaxed when breathing
You may want to really squeeze the yoga block depending if we’ve done an assessment
Use a chair at home if you’re struggling to feel hamstrings
WHY DO THIS?
Potentially decrease stress and global muscle tone (down regulate the central nervous system)
Loosen up your back and neck
Learn to maintain internal pressure throughout thorax and abdomen
Decrease anterior pelvic tilt
Start with 3 sets of 5 breaths (exhale + inhale)
Bear Hold Isometric
EQUIPMENT:
Your floor
(Optional) Wall or box
SET-UP:
Go down to the floor on your hands and knees
(Optional) put your feet flush against the wall
Place the hands directly under the shoulders and knees directly under the hips
Tuck your back pockets toward the back of your knees (posterior pelvic tilt)
Press heels back into the walls
Reach the knobby bone at the base of your neck (C7) toward the ceiling (scapular protraction)
Exhale ribs down and back (feel abs)
Maintain set up throughout execution
EXECUTION:
Maintaining set up, put majority of your body weight into the hands
Lift your knees about 1-2 inches off the floor
Hold the exercise for allotted time
Repeat for recommended sets and reps
ADDITIONAL TIPS:
Maintain heels firmly pressed into the wall
Press thumbs and index fingers into the floor and exhale every spit of air out to feel A LOT of abs
Keep your neck and face relaxed
WHY DO THIS?
Promote ribcage and pelvis positioning
Strengthen abdominals and serrates musculature
Start with 3 sets of 30” holds
The primary goal of these two exercises is to achieve a posterior pelvic tilt that sits stacked below the cranium. This can allow for the brain’s perception of where it is in space to readjust, while also promoting new length-tension relationships of the targeted musculature. Think about these exercises as full-body PNF with some true diaphragmatic breathing sprinkled on top.
Vision & Balance Exercises
Eye Isometrics
EQUIPMENT:
Your thumb or a pen
EXECUTION:
Move to each corner of your visual field without moving your head and hold for 5-20”
WHY DO THIS?
Strengthen your eye muscles
Reduce eye strain and focal vision
Improve peripheral vision
Vestibular & Vision Training
EQUIPMENT:
Your thumb or a pen
Some paper or sticky note
EXECUTION:
Move eyes, head, and neck in different directions
WHY DO THIS?
Strengthen your eye muscles
Reduce eye strain and focal vision
Improve peripheral vision
Stimulate ear canals
Challenge balance and kinesthetics
The primary goal of these visual and vestibular exercises is to reset these systems. As we sit in on spot and focus our vision on a single focal point, things get stuck. Moving things around can help assist some of our more biomechanically based breathing exercises while also improving our brain’s ability to sense our environment. These are pretty general exercises and you typically need more specific assessment to really dive into visual and vestibular training. But these exercises are a nice “shotgun” approach to supplement your posture practice.
Summary
Well I probably overloaded you during this post, but let’s review.
We now know that kyphosis is the normal curvature of the spine whereas hyperkyphosis is an excess curvature.
Essentially, forward head, rounded shoulders, and hyperkyphosis can be grouped under the umbrella term “upper cross syndrome” as they’re postures that can occur together.
Upper cross syndrome, as well as other postural deficits, are an exaggeration of our normal spinal curvatures and can occur due to…
Lack of motor control of the pelvis (anterior pelvic tilt)
Hyperactivity of the visual (eyes) system and vestibular system (ears/balance)
Having upper cross syndrome can have some adverse effects such as…
Winged scapula
Scapulohumeral rhythm issues
Cause even more hyperactivity of the vestibular/visual system (kind of a positive feedback loop)
We can fix our upper cross syndrome 70%-80% of the time (in my experience) with typical breathing exercises like the 90-90 hip bridge and bear isometrics. But sometimes, to really make things stick, we have to influence your visual and balance systems.
Need help improving your posture? Have a weird, nagging pain-thing going on that just won’t go away? Or maybe you’re bored with your current exercise plan and want to move better and get swole.
I can help!
Schedule a free meeting with me!
Citation:
Azadinia, Fatemeh MSc*; Kamyab, Mojtaba PhD, MSc, CPO(ir)*; Behtash, Hamid MD†; Ganjavian, Mohammad Saleh MD‡; Javaheri, Masoud R. M. MD§ The Validity and Reliability of Noninvasive Methods for Measuring Kyphosis, Journal of Spinal Disorders and Techniques: August 2014 - Volume 27 - Issue 6 - p E212-E218
Fedorak, Christine, MD; Ashworth, Nigel, MBChB, MSc, FRCPC; Marshall, John, BScPT, MSc; Paull, Heather, DC Reliability of the Visual Assessment of Cervical and Lumbar Lordosis: How Good Are We?, Spine: August 15, 2003 - Volume 28 - Issue 16 - p 1857-1859
Honda, J., Chang, S. H., & Kim, K. (2018). The effects of vision training, neck musculature strength, and reaction time on concussions in an athletic population. Journal of exercise rehabilitation, 14(5), 706–712.
Morningstar, M. W., Pettibon, B. R., Schlappi, H., Schlappi, M., & Ireland, T. V. (2005). Reflex control of the spine and posture: a review of the literature from a chiropractic perspective. Chiropractic & osteopathy, 13, 16. https://doi.org/10.1186/1746-1340-13-16
Singla, D., & Veqar, Z. (2017). Association Between Forward Head, Rounded Shoulders, and Increased Thoracic Kyphosis: A Review of the Literature. Journal of chiropractic medicine, 16(3), 220–229.
Yang, Hoesong, & Bae, Sea-hyun. (2013). The effect of shortening of small pectoral muscles on muscle activity of dorsal and large pectoralis muscles. Korean Journal of Integrated Medicine, 1 (4), 85–92.